口腔内化膿性肉芽腫の診断と治療:一連の症例|Revista Odontológica Mexicana
はじめに
化膿性肉芽腫は、口腔や皮膚の組織における非腫瘍性の増殖である。 その組織学的特徴は、炎症性浸潤と大きな血管新生能力を持つ肉芽組織の増殖である。これらの理由から、通常、異なる直径の血管新生が存在し、これらの形成は、組織内で突然の発症と完了を示す1。 組織学的に見ると、この病変は2つのグループに分類されます。毛細血管が薄いコラーゲン帯に囲まれた肉芽組織の小葉に組織化されていることがわかると、「毛細血管小葉状血管腫」と呼ばれ、一方、血管形成が組織内で明らかに秩序なく絡み合っていると、「非小葉状毛細血管腫」と呼ばれます2
このタイプの病変の病因についてはまだあまり明らかではありません。 2
この種の病変の病因はまだよくわかっていません。低度の刺激に反応する病変と考えられており、その中には、繰り返しの外傷、攻撃、ホルモン因子、特定の薬剤などが含まれます。 妊娠中にこの病変の発生率が高いのは、エストロゲンやプロゲステロンの濃度が高いことと関連している。2
過形成反応性病変は、口腔疾患に非常に頻繁に見られる。 Kadehは、30.4歳(±14.9歳)の患者において、化膿性肉芽腫が歯肉反応性病変全体の37%を占めると決定しました3
Epivatianosらは、女性に高い有病率(1:1.5)および全体の16%において局所病因が存在することを報告しました4。
臨床的観点から、化膿性肉芽腫は軟らかく急速に成長する腫瘤として現れ、おそらく小葉状で、表面サイズが変化し、赤みを帯びた色合いをしていることがあります。 2 主な部位は歯肉である(全症例の75%)。 口唇、舌、口腔粘膜、口蓋に生じることは少ない。 病変は、上顎の前歯部や歯肉の前庭部に多くみられます。 1,2
従来、この種の病変に対する治療は、骨膜下掻爬を伴う外科的全切除が選択されてきました。
症例提示症例1
全身的に健康な34歳の女性患者は、3.4と3.5の歯の隣にある歯肉の病変のために、San Martin de Porres大学の歯周病マスターズクリニックに紹介されました。 患者は約1年前に出血性歯肉増殖症が発生し、当時は切除術で治療したことを知らせてきた。 徐々に新しい病変が大きくなり、病変が咬合平面まで達したため、食事や歯磨きの際に違和感と出血があると報告されました。
臨床検査では、3.4と3.5の歯の高さに炎症性の歯肉病変が見つかりました。 大きさは約15 x 9mm。 病変は前庭側歯冠を覆い、硬く、小葉状で、粗い感触で、刺激により出血しました(図1、図2)。 歯周病評価では歯周ポケットは認めず、プラークの存在を認め、O’Leary口腔衛生指数は18.75と判定された。 X線写真では、3.4と3.5の歯間接触がなく、歯間部には修復物がありました(図3)

病変の正面。

Occlusal view of the lesion.

Periapical X-ray of the lesion area. Absence of interproximal contact between teeth 3.4 and 3.5.
Presumptive diagnosis: pyogenic granuloma.
Treatment: a first session of oral hygiene instruction was conducted, followed by supra-gingival scraping.
An excisional biopsy of the lesion was taken during the second session (Figure 4). The lesion was removed during this intervention as well as a healthy tissue margin and adjacent periosteum. For histopathological examination, a sample was taken, and transported in 10% formaldehyde. After this, soft tissue was recontoured (gingivoplasty) (Figure 5), and a periodontal cement pack was placed. Use of analgesic for 48 hours was prescribed, as well as 0.12% chlorhexidine rinses. Due to allergic reactions these rinses had to be discontinued after five days due to onset of ulcerative lesions at the level of attached gingiva.

Lesion excision.

Lesion removed.
Histopathological examination: 病理組織学的検査:試料は、偽上皮腫性過形成、固有層、内皮細胞でコーティングされた血管管、リンパ球、プラズマ細胞、組織球および時折多形核細胞からなる炎症性浸潤を示す、アカントフィック上皮で構成されていました(図6)。 これらの所見から臨床診断が確定した。
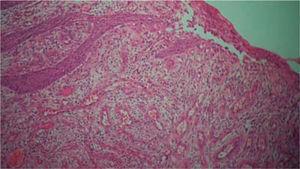
仮性上皮過形成を示す上皮、固有層、内皮細胞で被覆された血管管、リンパ球、形質細胞、組織球および時折の多形体からなる炎症性浸潤を示す上皮。
Controls: lesion volume decreased after a week, nevertheless, the area still exhibited a reddish hue, therefore, it was kept under observation (Figure 7). Two weeks later, a slight volume increase with whitish and reddish hue was observed, thus a relapse was suspected. At the third week decrease of tissue volume was observed without any presence of inflammatory signs.

Control visit after one week.
During a seven month follow-up suitable oral hygiene level was observed, no lesion relapse was observed (Figure 8).

ケース2
37歳の女性患者は、San Martin de Porres大学の歯周病マスタークリニックに相談をしにきました。 患者は、妊娠第2期に発症し、妊娠終了後9ヶ月間持続している歯肉病変の成長と出血を知らせてきました。
臨床検査では、歯1.1および2.1の部位に炎症性の歯肉病変が見つかりました。 病変の大きさは約9×9mmで、臨床的には歯冠の1/3を覆っていました。病変は無症状で、硬く、小葉状で、ゴツゴツした感触で、刺激により出血しました(図9)。 歯周病評価では歯周ポケットは認められませんでしたが、歯垢の存在が認められ、口腔衛生指数は50%(O’Leary)でした。

Lesion front view.
Radiographic examination revealed bone crest alteration between teeth 1.1 and 2.1 (Figure 10).

Periapical X-ray at the level of teeth 1.1 and 2.1. Presence of crest loss.
Presumptive diagnosis: pyogenic granuloma.
Treatment: fist session devoted to oral hygiene instruction followed by excisional biopsy of the lesion and gingivoplasty (Figures 11and12).

Lesion removal, extreme bevel incision.

Gingivoplasty.
Histopathological examination: sample composed of acanthic epithelium, pseudoepitheliomatous hyperplasia, lamina propria, vascular canals coated with endothelial cells, inflammatory infiltrate composed of lymphocytes, plasma cells, histiocytes and occasional nuclear polymorphs. These findings confirmed clinical diagnosis (Figures 13 and 14).
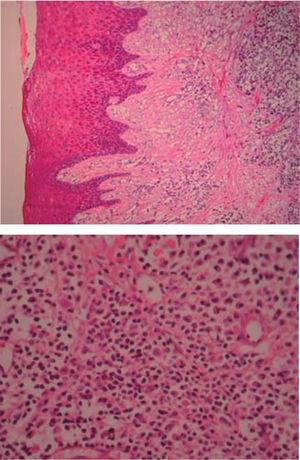
(HE 5x)アカントリック上皮、仮性上皮過形成、固有層、明らかな血管管および炎症性浸潤を認める。 (HE 10x)内皮細胞で被覆された血管管、リンパ球、形質細胞、組織球および時折核多形からなる炎症性浸潤
対照例:1週間後に病変部は縮小しましたが、赤みが残っていたため経過観察しました。 6ヶ月後、患者はより弱い強度(7×7mm)の再発を示した(図15)。 歯垢も同様に観察され、得られた口腔衛生指数(O’Leary)は52%であった。 An additional oral hygiene instruction session was conducted, with plaque removal and a second lesion excision. During this procedure, a greater margin of apparently healthy tissue was removed, reaching removal of periosteum adjacent to the lesion.

Lesion recurrence after six months.
Favorable evolution was observed in the next controls, oral hygiene levels were more satisfactory, lesion did not relapse up to a seven month follow up period (Figure 16).

症例3
全身健康な29歳女性は、上顎の前部分にある3年間の歯肉の病変により診察を受けました。 患者は、妊娠中に病変が発生し、痛みを伴わずに病変が進行していると報告した。 臨床評価では、23番と24番の歯の高さに約20mm×16mmの軟らかい可動性のある小児腫瘍が見つかりました。 腫瘍はピンク色を呈し、角化病巣を認めた(図17)。 歯周病評価では歯周ポケットが認められ、口腔衛生指数は78%であった(O’Leary)。 X線検査では、歯肉病変部に腋窩間石灰化を認めた(図18)。

Front view of the gingival lesion, located at the level of teeth 2.3 and 2.4.

Periapical X-ray, lack of bone loss.
Presumptive diagnosis: pyogenic granuloma.
Treatment: oral hygiene instruction was administered, followed by root scaling and planing, after which an excisional biopsy of the lesion was conducted (Figure 19) as well as a gingivoplasty procedure. Moreover, support periodontal therapy was recommended with periodontal maintenance sessions every three months during the first year.

Incision around the pedicle.
Histopathological examination: the sample exhibited pseudoepitheliomatous hyperplasia, lamina propria, vascular canals coated with endothelial cells, inflammatory infiltrate composed of lymphocytes, plasma cells, histiocytes and occasional nuclear polimorphs. These findings confirmed clinical diagnosis.
Controls: decrease of inflammatory circumstances of the wound area was observed after one week (Figure 20). Favorable evolution was observed in the following controls, more suitable oral hygiene levels were observed as well as lack of lesion recurrence, up to a six month follow-up period.

Control after eight days.
Case 4
A 46 year old female patient sought consultation due to a gingival lesion located at the level of teeth 1.3 and 1.4. The patient informed she was not under any drug or hormonal regimen.
Clinical examination revealed an inflammatory gingival lesion around teeth 1.3 and 1.5, measuring 9 x 9 mm approximately and covering a third of the clinical crown. The lesion was asymptomatic, firm, lobulated, smooth and bleeding on stimulus (Figures 21and22).

Front view of the lesion.

Lateral view of the lesion.
Periodontal evaluation revealed presence of plaque and calculus, as well as a 50% oral hygiene index (O’Leary). Patient exhibited a caries lesion in the distal aspect of tooth 1.3.
Presumptive diagnosis: pyogenic granuloma.
Treatment: oral hygiene instruction session and excisional biopsy with gingivoplasty (Figure 23).

Wound after lesion removal.
Histopathological examination: pseudoepitheliomatous hyperplasia and granulation tissue, vascular canals coated with endothelium and ingurgitation of erythrocytes, inflammatory infiltrate with neutrophil and histiocyte predominance (Figures 24 and 25).
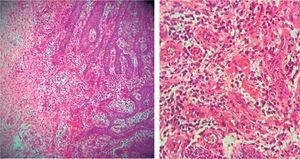
Pseudoepithelial hyperplasia and granulation tissue, vascular canals coated with endothelium and erythrocyte ingurgitation, inflammatory infiltrate with histiocyte and neutrophil predominance.
Controls: a reddish hue in the area was observed after one week, compatible with healing process.
症例5
27歳の健康な男性患者は、歯3.3および3.4の高さにある歯肉の病変のために受診しました。
臨床検査では、約9×9mmの大きさの炎症性歯肉病変が、臨床冠の舌側および前庭部を部分的に覆っていることが判明しました。 病変は硬く、滑らかで、小葉状でした(図26と27)。 歯周病評価では、プラークと石灰質の存在、および40%(O’Leary)の口腔衛生指数が認められました。

病変部の正面図。

Occlusal view of the lesion.
Treatment: oral hygiene instruction and excisional biopsy with gingivoplasty.
Histopathological examination: acanthic epithelium, showing pseudoepitheliomatous hyperplasia, lamina propria, vascular canal coated with endothelial cells, inflammatory infiltrate composed of lymphocytes, plasma cells, histiocytes and occasional nuclear polymorphs.
Controls: suitable evolution and healing wound were observed after one week. Five months later, no lesion recurrence was observed.
Discussion
Pyogenic granuloma is an inflammatory hyperplasia formed as a result of an exaggerated reaction of connective tissue to some localized minor lesion or any underlying irritation. 刺激因子には、歯石、口腔衛生不良、特定できない感染症、および過矯正修復がある。1,5-11 この刺激により、下層の線維-血管結合組織が過形成となり、肉芽組織の増殖が起こり、化膿性肉芽腫の形成につながる1,4。 化膿性肉芽腫の診断には、思春期や妊娠中のホルモンの変化、ある種の薬剤の投与、ある種の外傷などの要因を考慮する必要があります1,4,5。
この症例報告では、妊娠、近位接触がないなどの局所的要因、結石の存在、および口腔衛生状態の悪さとの関連で、化膿性肉芽腫の存在が記述されています。
組織学の観点から、化膿性肉芽腫には2種類あります。 このタイプのPGは、小葉状毛細血管腫(LCH)と呼ばれます。 第二のタイプ(非 LCH)は、肉芽組織に似た血管の増殖からなる。 非LCHの中心部と比較すると、LCHの小葉部には小径の毛細血管が多量に存在する。 化膿性肉芽腫の顕微鏡観察では、肉芽組織に似た大きな血管増殖が認められ、内皮線維性ストロマを形成する組織が見られ、太い内皮細胞で覆われた毛細血管が多く見られます。 層状上皮は過形成、菲薄化、潰瘍化することがある。 11
治療に関して、Powellは、他の外科的手法と比較して出血のリスクが少ないことから、この病変を切除するためにNd YAGレーザーを使用することを説明しています1
Vermaら6人は、従来の治療に反応しなかった肉芽組織の塊にフラッシュランプ励起パルス色素レーザーを使用することを報告し、組織が良好な反応を示すという結論に達しています。 Tayら13は、フラッシュランプ励起パルス染料レーザーによる治療の3年間のフォローアップ後、1回の治療で25%の患者が再発し、2回で40%、3回で30%、6回で5%と報告しました。
IshidaとRamos-Silva14は、化膿性肉芽腫治療に非常に役立つ技術として冷凍外科を説明し、その柔らかさと湿気のために口腔粘膜がこの技術に最適の場所だと報告しています。 一方、Ghodsi15 は、外科的切除を 1 回で行い、再発が 0%であった治療法と、クライオサージェリーを 1 回で 63%、2 回で 32%、3 回で 5%の患者に行い、再発が 0%であった治療法を比較しています。 松本ら16は、硬化物質としてオレイン酸モノエタノールアミンを用いて1回で治療したところ、再発は0%であった。
しかし、現在までのところ、多くの報告では外科的切除が治療法として選択されている。 病巣切除後、下層組織の掻爬を行い、周辺部や骨膜を含む深さで2mmのマージンをとって切除することが推奨されています。 さらに、化膿性肉芽腫の発症に関連する可能性のある異物、結石、修復物を除去する必要があります。
Al Khaleebら3は12年間の追跡調査の結果、骨膜除去を伴う外科的切除を行い、さらに隣接骨組織のキュテージを行うと再発するケースが5.8%と報告しています。 17,18
以上のことから、正確な診断には、臨床症状の観察、患者の全身状態の詳細な臨床歴、過剰な組織反応とそれに続く化膿性肉芽腫の形成を刺激する局所因子を確認することが重要であることが推奨できる。 臨床診断は常に組織学的検査で確認する必要がある。 今回の症例では、口腔衛生状態が最も重要な要因の一つであったため、化膿性肉芽腫の治療には理学療法を第一に考えなければならない。
異なる研究により、高い成功率と低い再発率を持つ異なる治療技術が評価されていることも同様に観察されています。これらの技術は、従来の外科的切除と同様に、凍結手術、フラッシュランプ励起パルスダイレーザーです。 しかし、外科的切除は基本的な手術器具を用いて1回で行うことができるため、数回の手術と特別なトレーニングや器具を必要とする他の手法とは対照的であることを考慮する必要があります。 この技術は、日常臨床に容易に適用することができ、患者さんにとってより快適なものとなります。